Major Medical Conditions: Expenditure Analysis
By Daniel Montanera, Ph.D., Assistant Professor, Department of Economics, Seidman College of Business, Grand Valley State University
This analysis provides general cost information about some of the most prevalent and expensive medical conditions. This section’s purpose is to identify and track trends in health care expenditures for selected chronic health conditions and to examine geographic differences in the cost of care. The data presented in this section are average annual member expenditures, including prescription medication expenditures, for those enrolled in private health insurance plans administered by Blue Care Network (BCN), Blue Cross Blue Shield of Michigan (BCBSM), and Priority Health (PH) for the years 2022-2023. [1] The following factors should be considered when interpreting analyses in this section:
- Differences in benefit structures and enrollment. Both BCN and PH offer primarily HMO products while BCBSM members are predominantly enrolled in PPO plans. HMOs tend to operate through selective contracting and provider referrals, utilizing networks in order to achieve cost savings. PPOs tend to have fewer restrictions on members seeking care and, therefore, usually require additional member cost-sharing in the form of higher premiums, higher coinsurance rates, or higher copays. Because of these differences in benefit structures, evidence suggests that HMO plans are more attractive to enrollees who are healthier, who have less complex medical needs, or who have no longstanding ties to particular providers (Ji and Liu, 2007; Nicholson et al., 2004; Tchernis et al., 2006). However, some research has failed to find a substantial difference in health status for those enrolling in HMO plans (Schaefer and Reschovsky, 2002). Furthermore, enrollment changes can alter the underlying disease burden of the payer mix resulting in changes in utilization and expenditures.
- Disease selection. The health status, and thus the expenditures, for members with specific conditions might vary due to differences in demographics and health behaviors. For example, patients in some counties insured by one payer may be sicker than patients in other counties who are insured by a different payer.
- Expenditures beyond disease. In each case, the average patient expenditure data is for services not only related to the specific disease in question, but also for other unrelated medical costs the member may have incurred during the year. Differences in expenditures or treatment intensity for these unrelated health issues can result in additional variation in average patient expenditure estimates. Expenditure estimates from each insurer can vary considerably because of these factors. Thus, we average the data for all three insurers to arrive at a more robust estimate of member expenditures.
KOMA Region Expenditures
As we have done in previous versions of this publication, we choose to focus on six chronic conditions that are associated with high prevalence rates and high levels of resource utilization: asthma, coronary artery disease (CAD), depression, diabetes, hyperlipidemia, and low back pain. For comparison, we also include “healthy members,” which we define as those between the ages of 30 and 39 who had not been diagnosed with any of the six chronic conditions previously listed and who have total annual expenditures below $450,000. Figure 1a provides the average annual expenditures per member for each of these conditions in Kent, Ottawa, Muskegon, and Allegan (KOMA) counties in 2022 and 2023. In most cases, we identified members in each disease category according to specifications defined by the Healthcare Effectiveness Data and Information Set (HEDIS). We excluded Medicaid and Medicare enrollees from our expenditure estimates. Finally, all expenditure estimates in Figure 1a are reported in 2023 dollars.
Figure 1a: Average Expenditures per Member in KOMA, 2022 - 2023
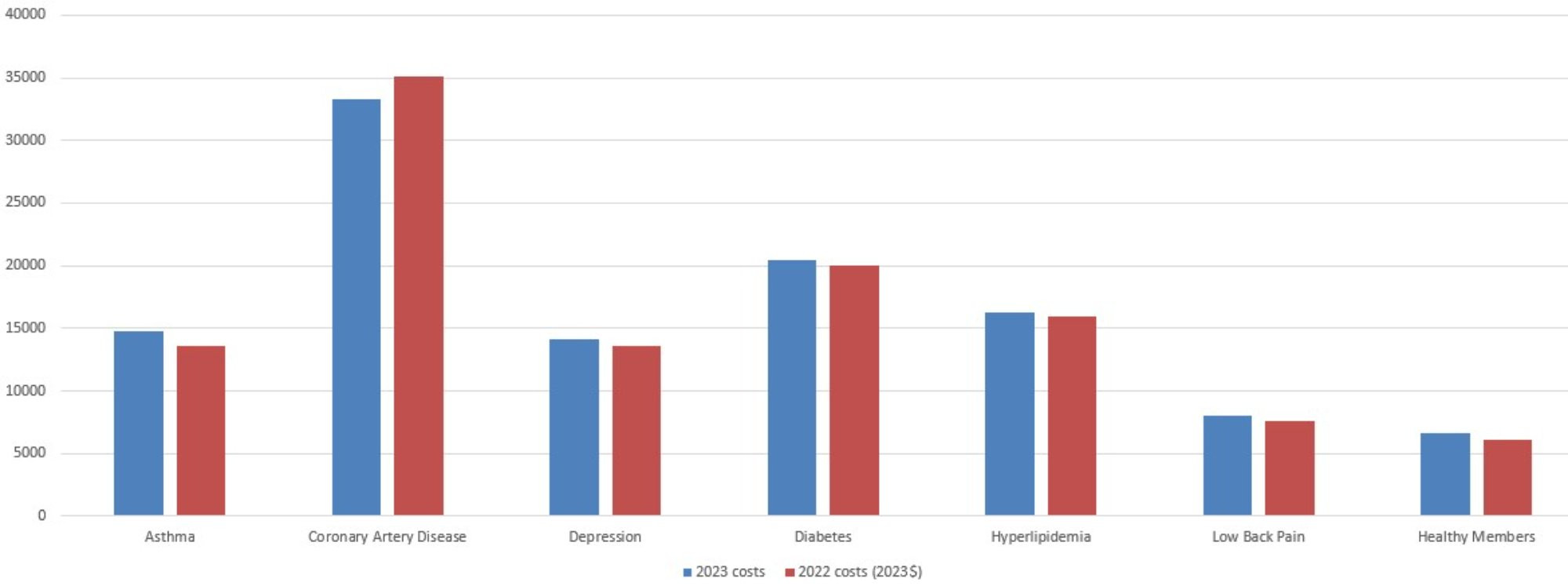
Description: The Average Expenditures per Member in KOMA, 2022-2023 graph shows average insurer expenditures for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members, for 2022 and 2023. In general, expenditure has risen slightly.
Source: BCBSM, BCN, and Priority Health member data (2024).
Figure 1a indicates that, after adjusting for inflation, expenditures in KOMA increased for five of the chronic conditions from 2022 through 2023 and decreased for only one: CAD. This is nearly the opposite of the findings from last year’s report, where real expenditures declined for most of the conditions. This was largely due to high inflation in 2022, however, and with the slower rate of inflation in 2023, this effect is not so pronounced. Figure 1b further highlights the percentage change in average member costs. Here, we note that real expenditures increased for asthma (+8.7 percent), healthy members (+8.3 percent), low back pain (+4.8 percent), depression (+3.4 percent), hyperlipidemia (+2.6 percent), and diabetes (+1.8 percent). Expenditures decreased for CAD (-5.4 percent). In dollar terms, the greatest average per-member changes in expenditure were seen in asthma (+$1,180) and CAD (-$1893). Unfortunately, we are unable to identify the cause of these changes in spending.
Figure 1b: Percentage Change in Average Member Costs 2022 - 2023
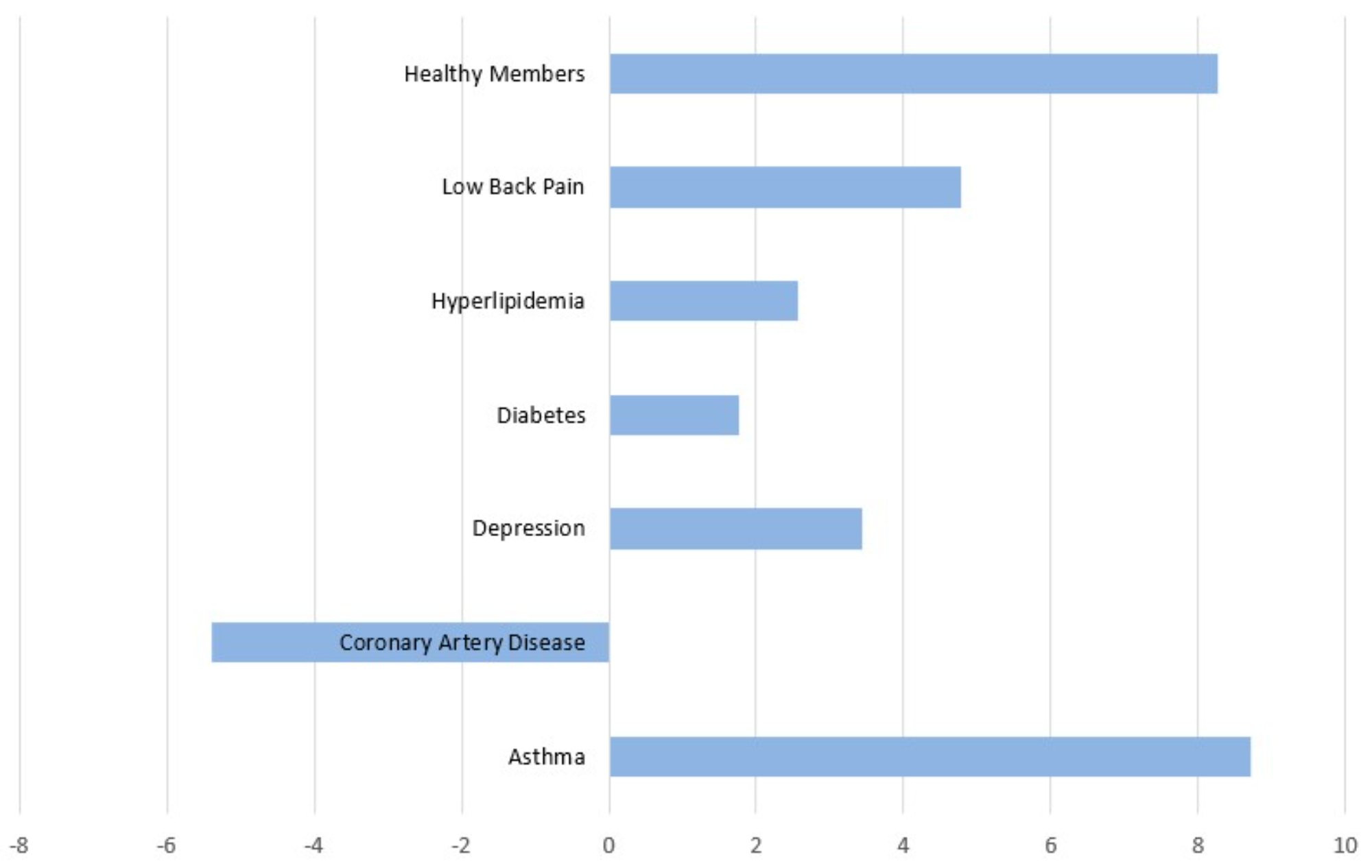
Description: The Percent Change in Average Member Costs in the KOMA Region, 2022-2023 graph shows the percent change in average insurer expenditures for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members, from 2022 to 2023. In general, expenditure has risen slightly.
Source: BCBSM, BCN, and Priority Health member data (2024).
The disease-specific shares of expenditure related to prescription drugs are presented in Figure 2. This figure returns after being removed from last year’s report due to irregularities in that year’s data. As a result, the figure compares 2023 prescription drug spending shares with those of 2021, skipping the year for which the data was unreliable. The prescription drug share of total spending for 2023 ranges from 22 percent for members with CAD to 48 percent for those diagnosed with asthma. We note that prescription drug expenditure’s share of overall disease-specific expenditures rose from 26 to 33 percent in real terms across all conditions over the two years. In dollar terms, average real prescription drug expenditures increased between 2021 and 2023 for members diagnosed with asthma ($774), diabetes ($628), CAD (+$562), hyperlipidemia (+$364), low back pain (+$341), and depression (+$152).
Figure 2: Rx Share of Average Expenditures per Member in KOMA, 2021 - 2023
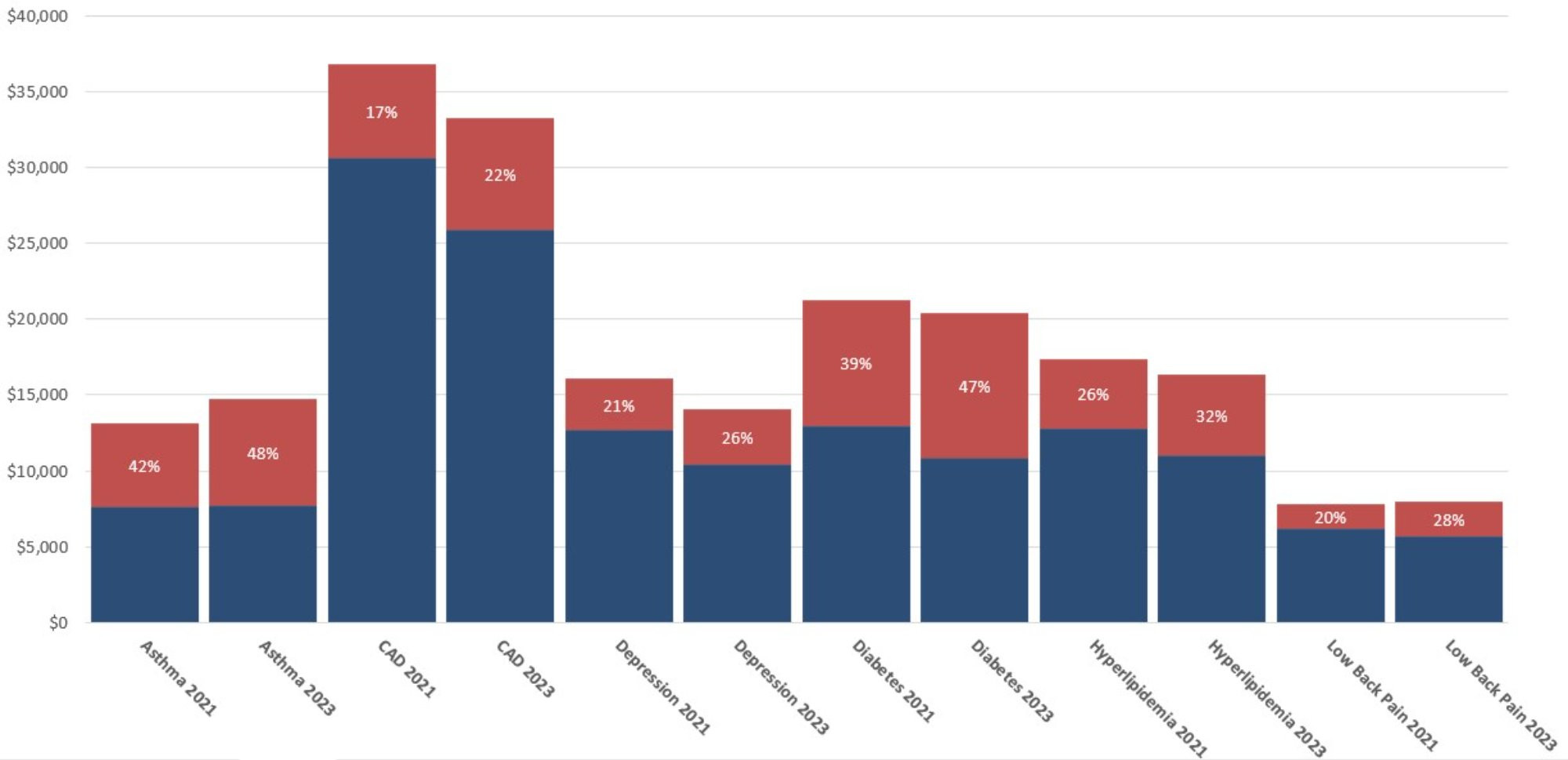
Description: The Rx Share of Average Expenditures per Member in KOMA, 2021 - 2023 graph shows the share of average insurer expenditures due to prescription drugs for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members, from 2021 to 2023. In general, shares have risen significantly.
Source: BCBSM, BCN, and Priority Health member data (2024).
Differences in Average Annual Expenditures Between KOMA and the Detroit Region
Figure 3a compares average annual per member expenditures in both the KOMA and Detroit regions. We define the Detroit region as Oakland, Macomb, and Wayne counties. Figure 3a indicates that 2023 average expenditures for all conditions and healthy members are higher in the KOMA region than in the Detroit region. This has not been the case in any version of this report prior to this year. The percentage differences vary across diagnoses, with healthy members’ expenditures in KOMA being 36 percent higher than Detroit while diabetes expenditures are only 4 percent higher. Differences in spending for the same condition between the east and west sides of the state may result from several reasons, including higher prices for care, economies of scale, greater use of medical services/technologies, or geographic differences in the underlying health of the population.
Figure 3a: Average Expenditures per Member, 2023
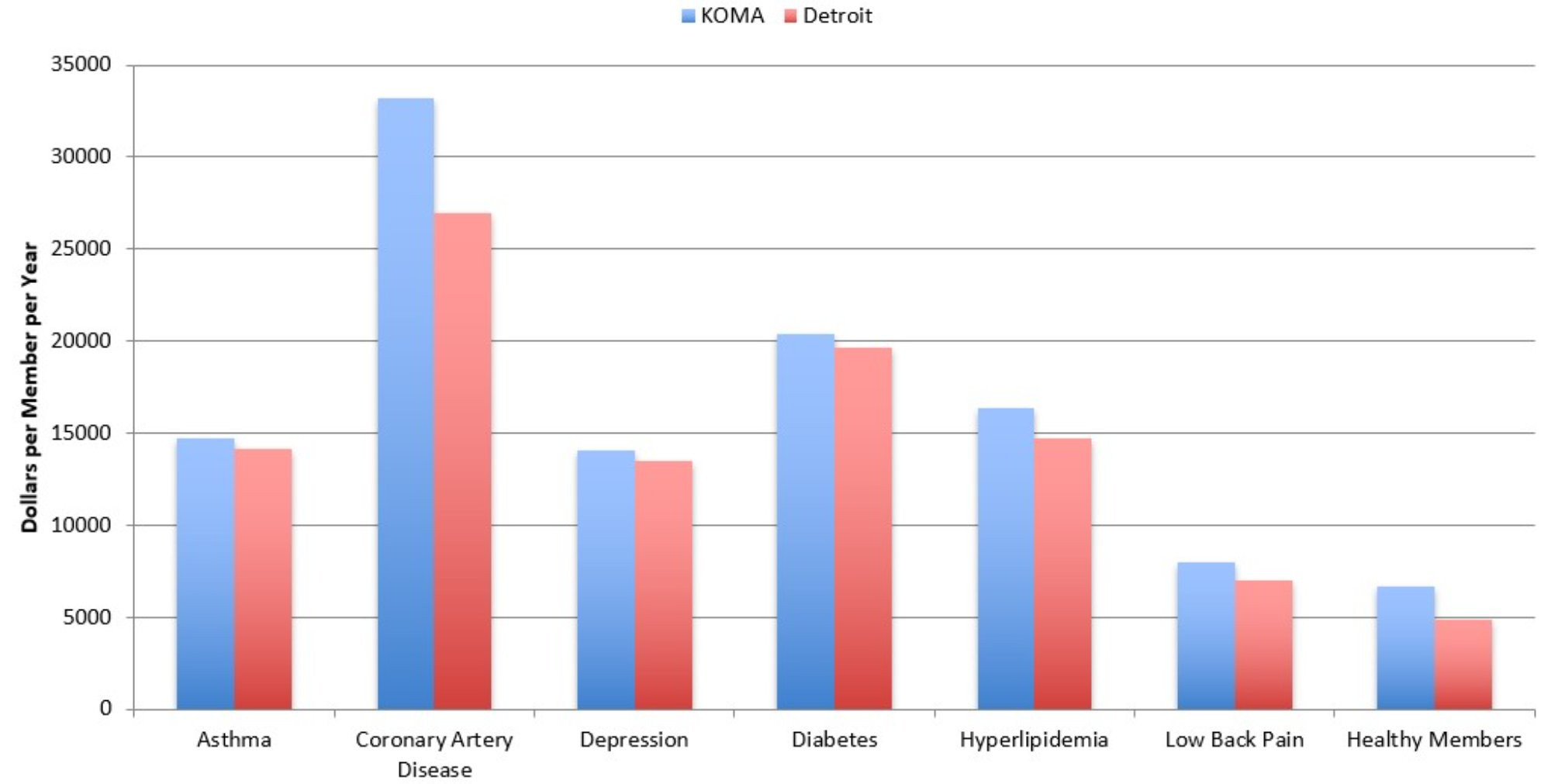
Description: The Average Expenditures per Member, 2023 graph shows the average insurer expenditures in both KOMA and Detroit regions for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members in 2023. For all chronic conditions, per member expenditure in KOMA is slightly higher than in Detroit.
Source: BCBSM, BCN, and Priority Health member data (2024).
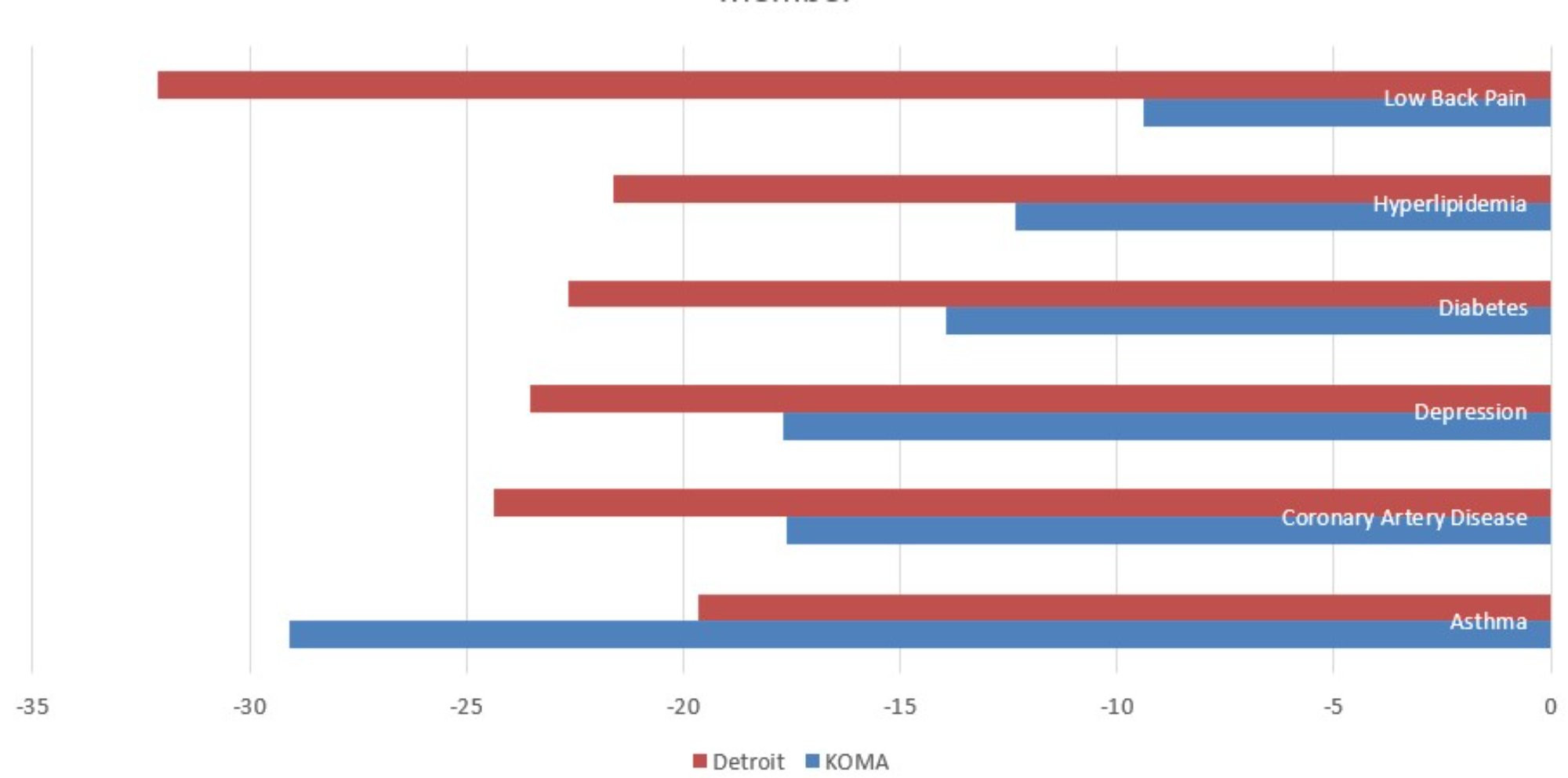
Figure 3b plots the percentage change in expenditures for each condition from 2022 to 2023. So, while Figure 3a provides differences in spending levels between the two regions, Figure 3b presents a more dynamic look at how those spending levels changed in the past year. On the whole, the figure shows that spending per member diagnosed with each of these conditions is moving in different directions on the two sides of the state. Apart from healthy members, expenditures decreased in Detroit across all conditions. Except for CAD, the opposite was true in KOMA. This was not true in the previous version of this report, where KOMA and Detroit regions experienced changes in expenditure in the same direction for most of the chronic conditions. The greatest disparity in expenditure changes involved low back pain, with a 16.8 percentage point difference in favor of Detroit. The smallest disparity involved CAD, with only a 4.7 percentage point difference in Detroit’s favor. The broad message from Figures 3a and 3b is that real expenditures across the chronic conditions tended to move in different directions between 2022 and 2023; rising in KOMA and falling in Detroit. Having greater per-member expenditures in KOMA for all five chronic conditions and healthy members is a source of concern for the region that is worth monitoring.
Figure 3b: 2022-2023 Percentage Change in Average Expenditures per Member
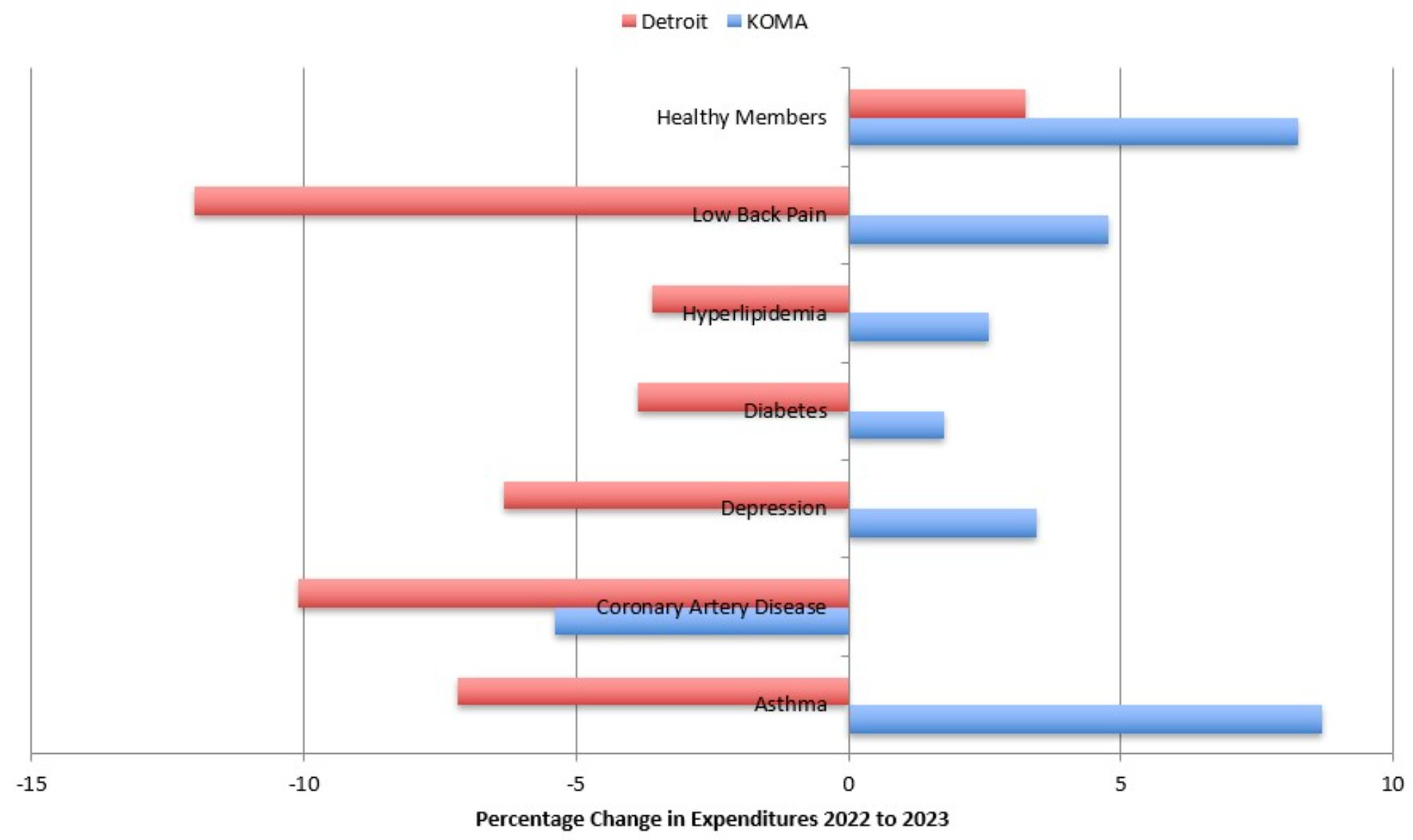
Description: The 2022-2023 Percentage Change in Average Expenditures per Member graph shows the percent change in average insurer expenditures in both KOMA and Detroit regions for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members, between 2022 and 2023. Expenditures tended to increase in KOMA and decrease in Detroit.
Source: BCBSM, BCN, and Priority Health member data (2024).
As was the case for the previous four years, we have access to the average risk scores of 2023 members, which allows us to adjust for expenditure differences between the KOMA and Detroit regions that are due to differences in the underlying health of their residents. Figure 3c reports two average member expenditure measures in KOMA across all conditions. The first measure is the actual (raw) KOMA expenditures as calculated for Figure 1a. The second is the predicted average KOMA region expenditures for these members if the KOMA risk scores were the same (on average) as those in the Detroit region, whose expenditures are also shown in the figure. Therefore, a comparison of the middle and right bars for each diagnosis reveals expenditure differences due to factors other than the wellness of the regional member populations.
The adjusted expenditures for the KOMA region in the middle columns of Figure 3c show that the spending disparities between regions are even more concerning than those identified in Figures 3b. Upon accounting for differences in the underlying health of members in the two regions, the spending gaps tend to be even more severe. Considering adjusted expenditures instead of raw, the KOMA region expenditures are higher than those of Detroit by 3.6 percent for asthma, 28 percent for CAD, 21 percent for depression, 14 percent for diabetes, 20 percent for hyperlipidemia, 23 percent for low back pain, and 34 percent for healthy members. The adjustment reveals that the KOMA region continues to have a relatively healthy population compared to Detroit, and so the differences in raw expenditures between the regions on members with the same diagnoses must be due to other factors. Figure 3c suggests there could be additional savings in KOMA from bringing prices or treatment approaches more inline with the Detroit region for all these conditions. It is not clear how this would affect access to or quality of care in the KOMA region, however, or how much of the difference in expenditure is due to economies of scale given Detroit’s larger population, and so additional investigation is necessary before a recommendation can be made.
Figure 3c: Average Expenditures per Member with Risk-Adjusted KOMA Values, 2023
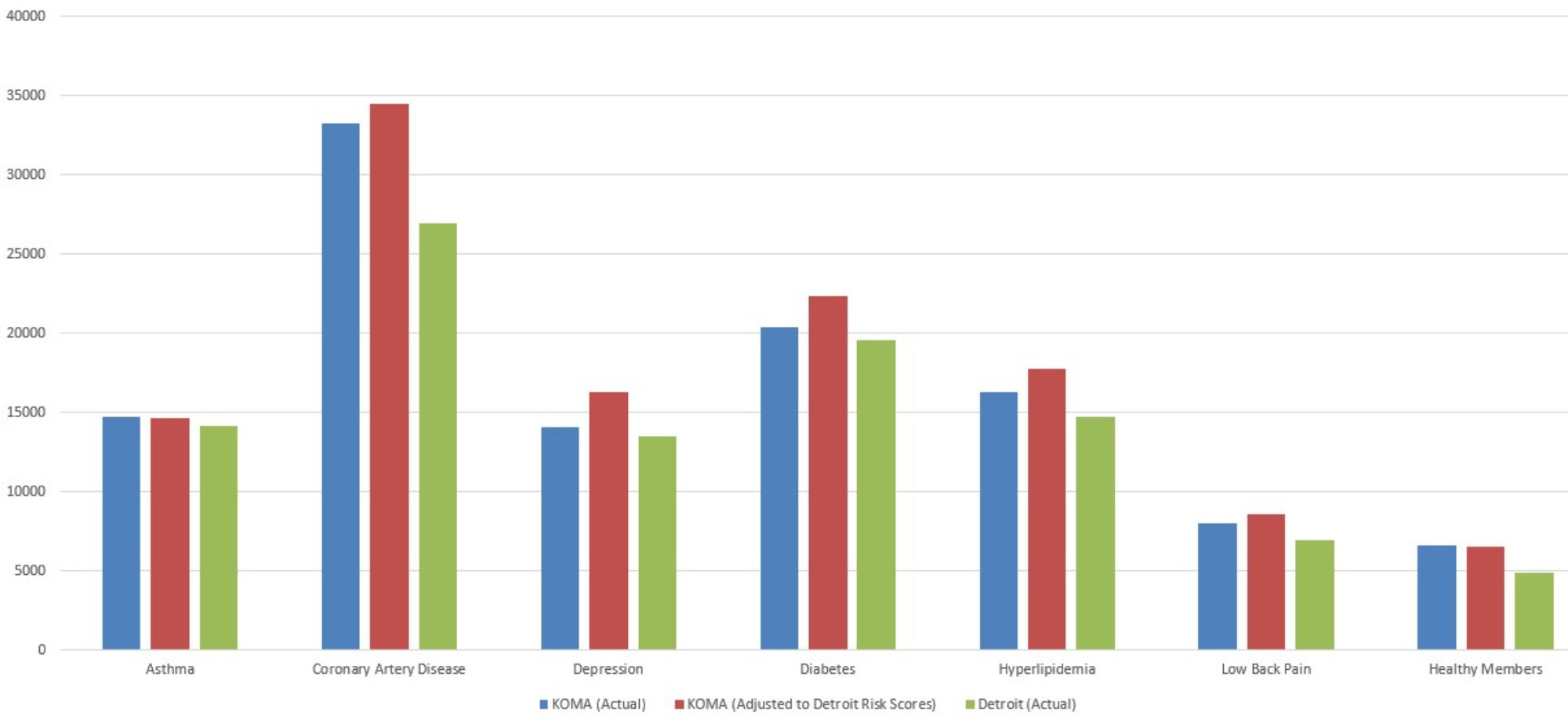
Description: The Average Expenditures per Member with Risk-Adjusted KOMA Values, 2023 graph shows the average insurer expenditures in both KOMA and Detroit regions, as well as a risk-adjusted version of KOMA’s, for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members in 2023. The risk-adjusted KOMA expenditures tend to be significantly higher than both the unadjusted KOMA and Detroit expenditures.
Source: BCBSM, BCN, and Priority Health member data (2024).
Health Services Use
Figures 4a through 4c examine regional differences in health care utilization for each of the six conditions. This is the eighth year that we have been able to include utilization data in our analysis, and this brings us closer to identifying the causes behind the documented expenditure growth.
Figure 4a displays the average number of annual inpatient visits for members in KOMA and the Detroit region in 2023. This figure is consistent with the previous three Health Check reports in showing that hospitalization rates tend to be higher on the east side of the state than the west. For example, members with diabetes experience an average of 0.11 inpatient admissions per year in KOMA, while those in Detroit average 0.17 hospital visits per year. This represents a small percentage point decline in the gap between 2022 and 2023. The other conditions, however, show that the gaps in inpatient visits shrinking rapidly. This is true for CAD (24 to 11 percent), depression (26 to 12 percent), hyperlipidemia (31 to 25 percent), and low back pain (27 to 2 percent). Only asthma showed an increase in the inpatient utilization gap (19 to 27 percent). While the trend of the last four years has tended to show a narrowing of the gap in inpatient visits between KOMA and Detroit, the narrowing accelerated in 2023. Should that continue, KOMA may lose its advantage over the Detroit region in inpatient utilization.
Figure 4a: Average Annual Inpatient Visits per Member, 2023
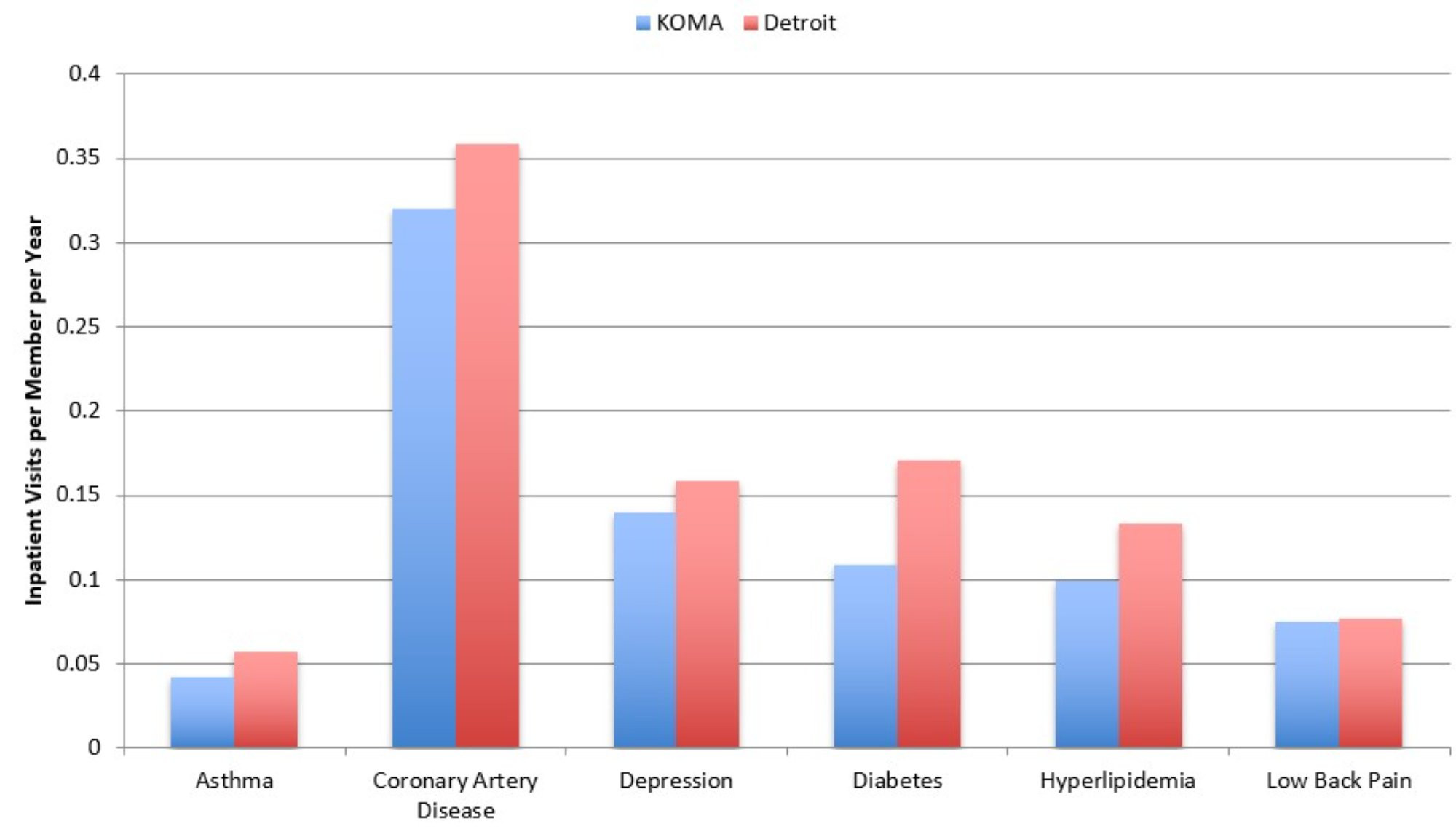
Description: The Average Annual Inpatient Visits per Member, 2023 graph shows the average annual inpatient visits per member in both KOMA and Detroit regions for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members in 2023. For all chronic conditions, inpatient visits per member are higher in Detroit than in Grand Rapids.
Source: BCBSM, BCN, and Priority Health member data (2024).
Figure 4b extends the utilization analysis to emergency department (ED) use. ED use was once again higher in the Detroit region than in KOMA for all six chronic conditions in 2023, just as it was in 2022. For example, those with a low back pain diagnosis average 0.57 ED visits per year in Detroit compared to 0.41 ED visits per year in the KOMA region (indicating that we observe approximately 26 percent fewer ED visits per member in KOMA for lower back pain than in Detroit). This gap was 34 percent in 2022, however, and so this figure continues to show evidence of narrowing gaps between the two regions in utilization of expensive forms of care. Similar results can be observed for the other conditions. While those in KOMA consumed 13.9 percent fewer ED visits per member with CAD than in the Detroit region in 2022, that difference has shrunk to 2.2 percent in 2023. A similar narrowing of gap is observed for asthma (17 to 14 percent), depression (24 to 17 percent), diabetes (22 to 14 percent), and hyperlipidemia (18 to 12 percent). Overall, per-member ED utilization clearly remains higher in the Detroit region than in the KOMA region for each of these diagnoses, though gaps have narrowed over the previous year. These per-member statistics appear at odds with the AHA Hospital Statistics data from Figure 4 of the Benchmarking Communities section, which found a widening gap in ED use between Grand Rapids and Detroit in 2022. The data used in Figure 4b is from one year later, however, and only reflects ED use among members enrolled with three private insurance plans and only for those with certain diagnoses. The discrepancy could be explained by emergency room use in KOMA declining among other types of patients not fitting into these categories (including the uninsured and those with public coverage).
Figure 4b: Average Annual Emergency Department Visits per Member, 2023
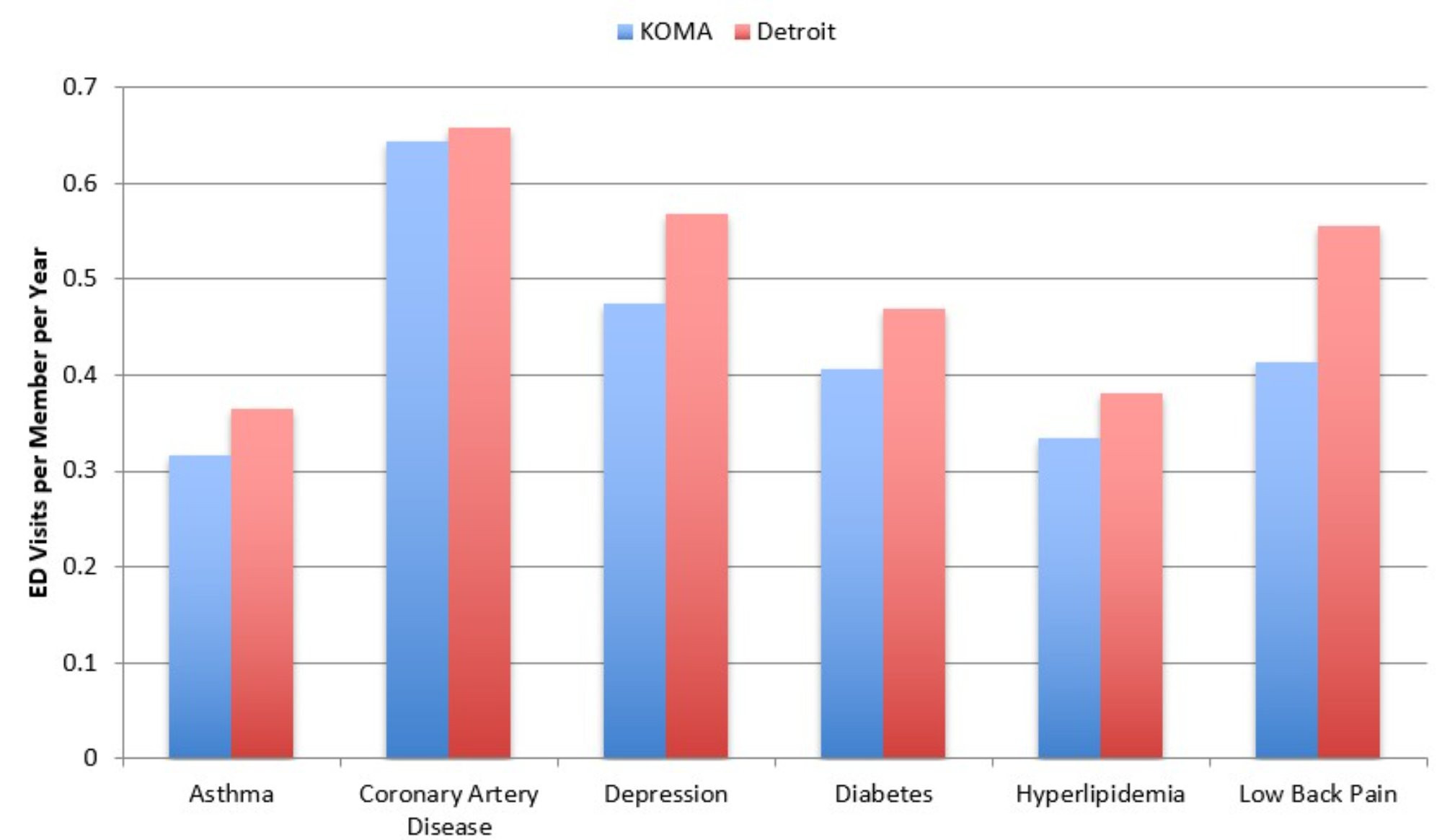
Description: The Average Annual Emergency Department Visits per Member, 2023 graph shows the average annual emergency department visits per member in both KOMA and Detroit regions for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members in 2023. For all chronic conditions, emergency department visits per member are higher in Detroit than in Grand Rapids.
Source: BCBSM, BCN, and Priority Health member data (2024).
Next, utilization in terms of prescription drug fills is presented in Figure 4c. As in the previous report, we find evidence of higher use rates in the Detroit region than in the KOMA region. For example, the average member with diabetes in the KOMA region had 65 prescription fills in 2023 compared to 70 for individuals with diabetes in the Detroit region. Assuming that each member filled a prescription 12 times throughout the year, then this would represent an average of approximately five distinct prescriptions for a person with diabetes in KOMA and just under six distinct prescriptions for one in Detroit. Beyond diabetes, we note an average of 7 percent fewer prescription fills in KOMA than in Detroit for members with a depression diagnosis (down from 12 last year), and similarly 9 percent fewer prescription fills in KOMA for members with a low back pain diagnosis (down from 15 percent). Therefore, just as for inpatient visits and ED usage, rates of prescription drug utilization are narrowing between the two regions.
Figure 4c: Average Annual Prescription Fills per Member, 2023
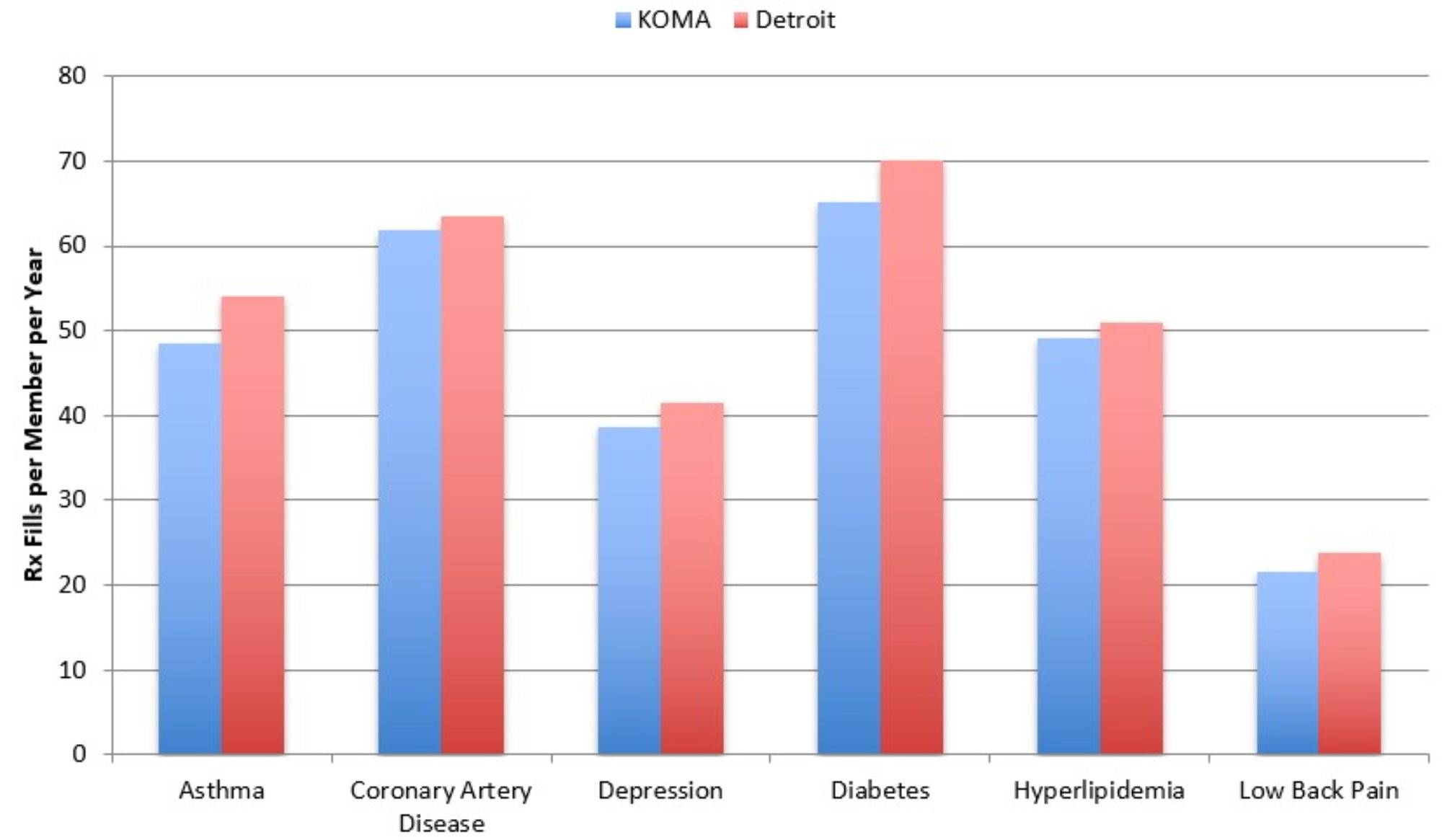
Description: The Average Annual Prescription Fills per Member, 2023 graph shows the average annual prescription fills per member in both KOMA and Detroit regions for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members in 2023. For all chronic conditions, prescription fills per member are higher in Detroit than in Grand Rapids.
Source: BCBSM, BCN, and Priority Health member data (2024).
Annual telehealth visits per member constitute the final utilization metric examined here, in Figure 4d. The Detroit region continues to utilize telehealth to a greater degree than the KOMA region across all six chronic conditions. Telehealth usage is now falling on both sides of the state.
Figure 4d: Average Annual Telehealth Visits per Member, 2023
Description: The Average Annual Telehealth Visits per Member, 2023 graph shows the average annual telehealth visits per member in both KOMA and Detroit regions for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members in 2023. For all chronic conditions, telehealth visits per member are higher in Detroit than in Grand Rapids.
Source: BCBSM, BCN, and Priority Health member data (2024).
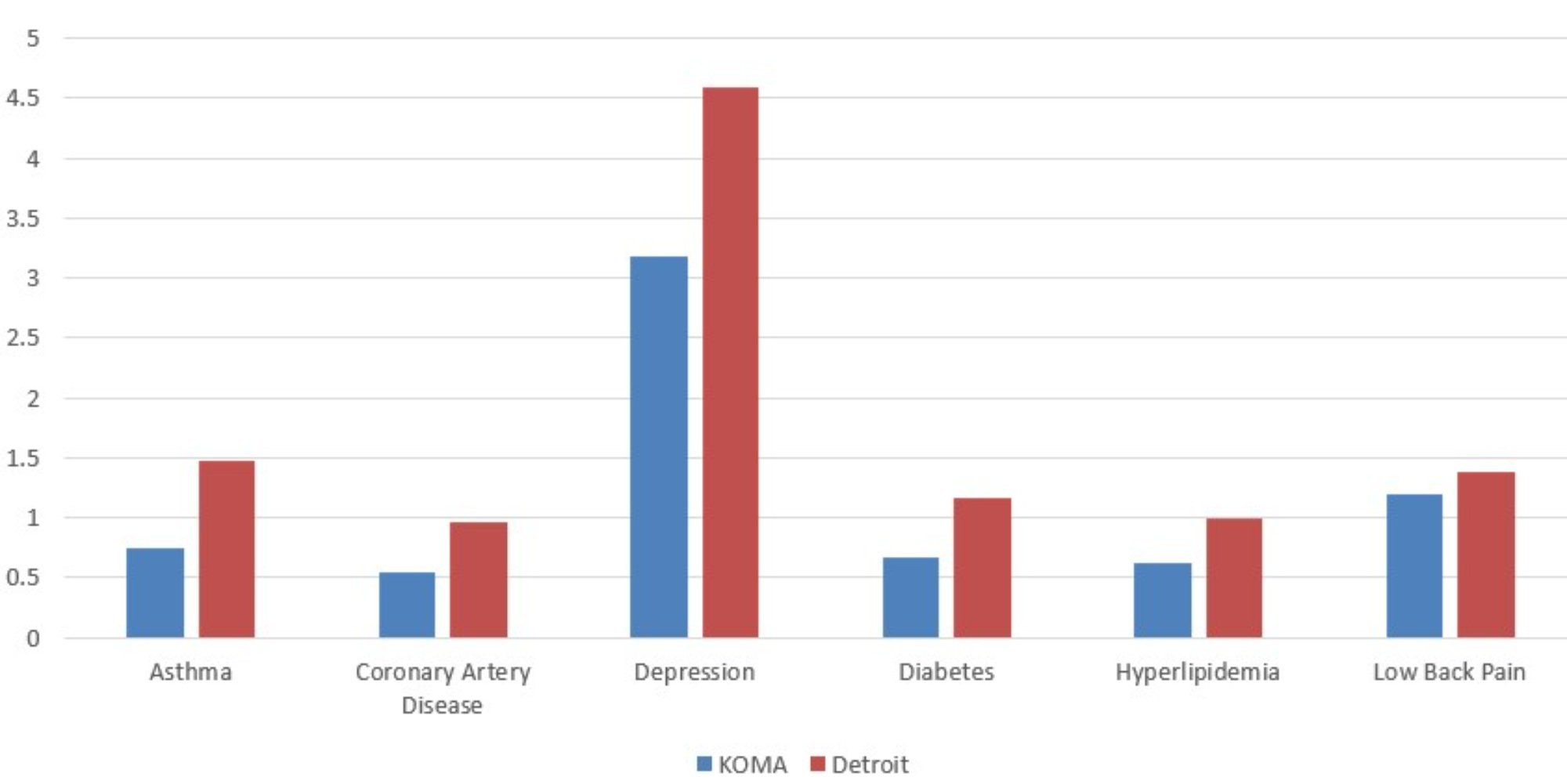
These declines, which can be observed in Figure 4e, show telehealth utilization falling faster in percentage terms in Detroit than in KOMA for all conditions except asthma.
Figure 4e: 2022-2023 Percentage Change in Average Telehealth Visits per Member
Description: The 2022-2023 Percentage Change in Average Telehealth Visits per Member graph shows the percent change in average annual telehealth visits per member in both KOMA and Detroit regions for each member diagnosed with one of six chronic conditions (asthma, coronary artery disease, depression, diabetes, hyperlipidemia, and low back pain) as well as for health members, between 2022 and 2023. For all chronic conditions, and in both regions, telehealth visits have declined, though more significantly in Detroit.
Source: BCBSM, BCN, and Priority Health member data (2024).
Comorbidities
In this section, we take a closer look at expenditures associated with diabetes and depression by examining the impact of additional diagnoses. Joint diagnoses and the presence of multiple comorbidities can lead to higher resource utilization and higher levels of spending. Importantly, we are not examining clinical linkages between these conditions, but rather only focusing on expenditure differences associated with multiple diagnoses. Figure 5a plots average annual member expenditures for those with only a diagnosis of diabetes, those with diagnoses of diabetes and asthma, diabetes and hypertension, diabetes and depression, and diabetes and CAD. According to Figure 5a, the addition of comorbidities greatly impacts the average expenditures associated with a diagnosis of diabetes. For example, expenditures in KOMA for a member diagnosed with diabetes and depression compared to a diagnosis of diabetes alone adds about $11,989 to the annual expenditure estimate, while a diagnosis of diabetes and CAD (instead of diabetes alone) adds $24,560 to the expenditure estimate. These are significantly lower differences for both combinations of diagnoses compared to previous years.
Figure 5a: Expenditures on Members with Diabetes and Comorbidities, 2023
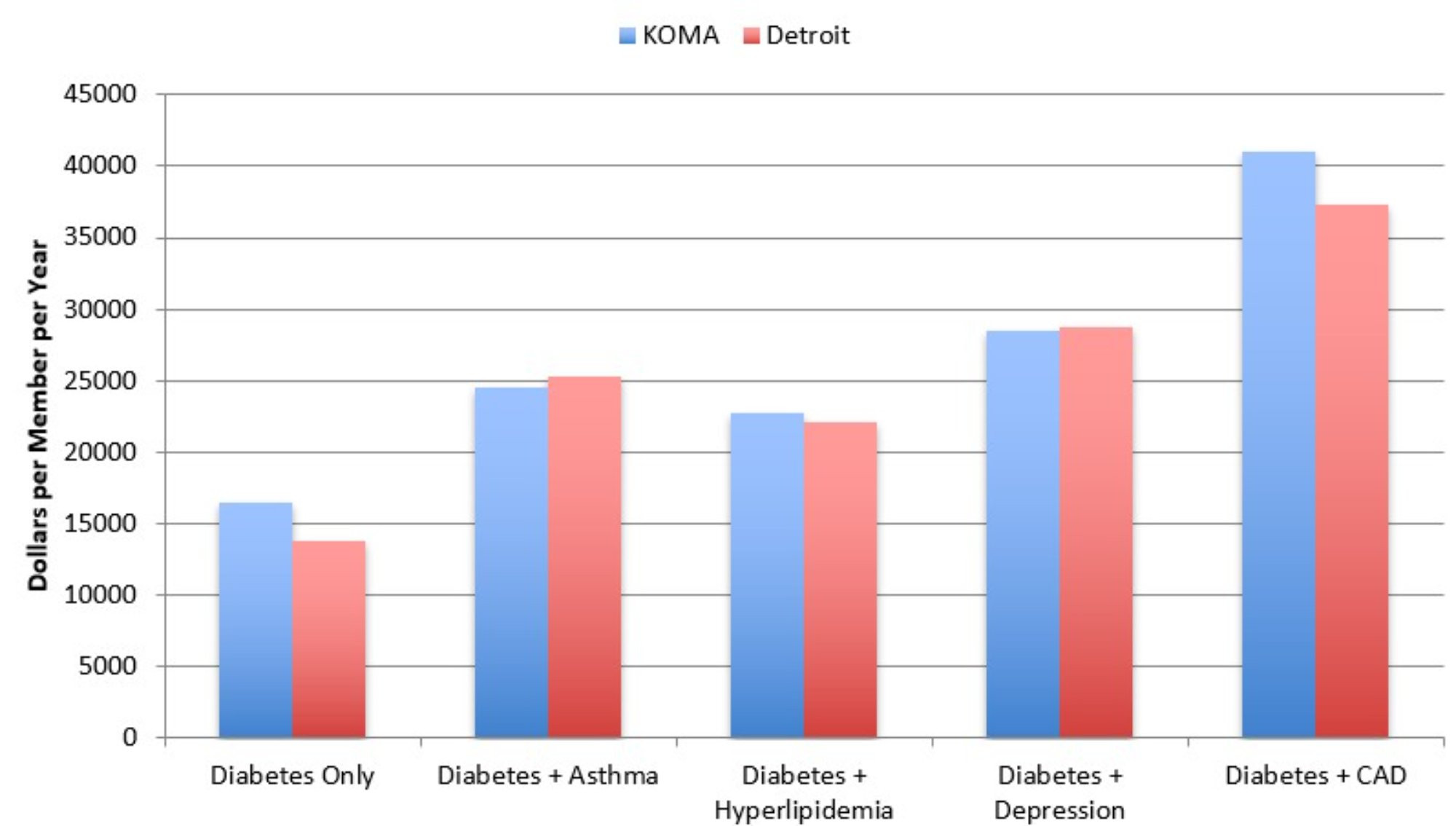
Description: The Expenditures on Members with Diabetes and Comorbidities, 2023 graph shows the average 2023 insurer expenditures in both KOMA and Detroit regions for each member with only a diabetes diagnosis, as well as diabetes in combination with asthma, hyperlipidemia, depression, and coronary artery disease. For both regions, combinations of conditions result in expenditure greater than for members with each condition separately.
Source: BCBSM, BCN, and Priority Health member data (2024).
Figure 5b displays the results of a similar analysis that focuses on depression. The results are consistent with those in Figure 5a: the presence of multiple conditions greatly increases average annual expenditures for members with depression. For example, expenditures in Detroit for a member diagnosed with depression and CAD compared to a diagnosis of depression alone adds about $33,186 to the expenditure estimate, which is a significant decline from the previous year.
Figure 5b: Expenditures for Members with Depression and Comorbidities, 2023
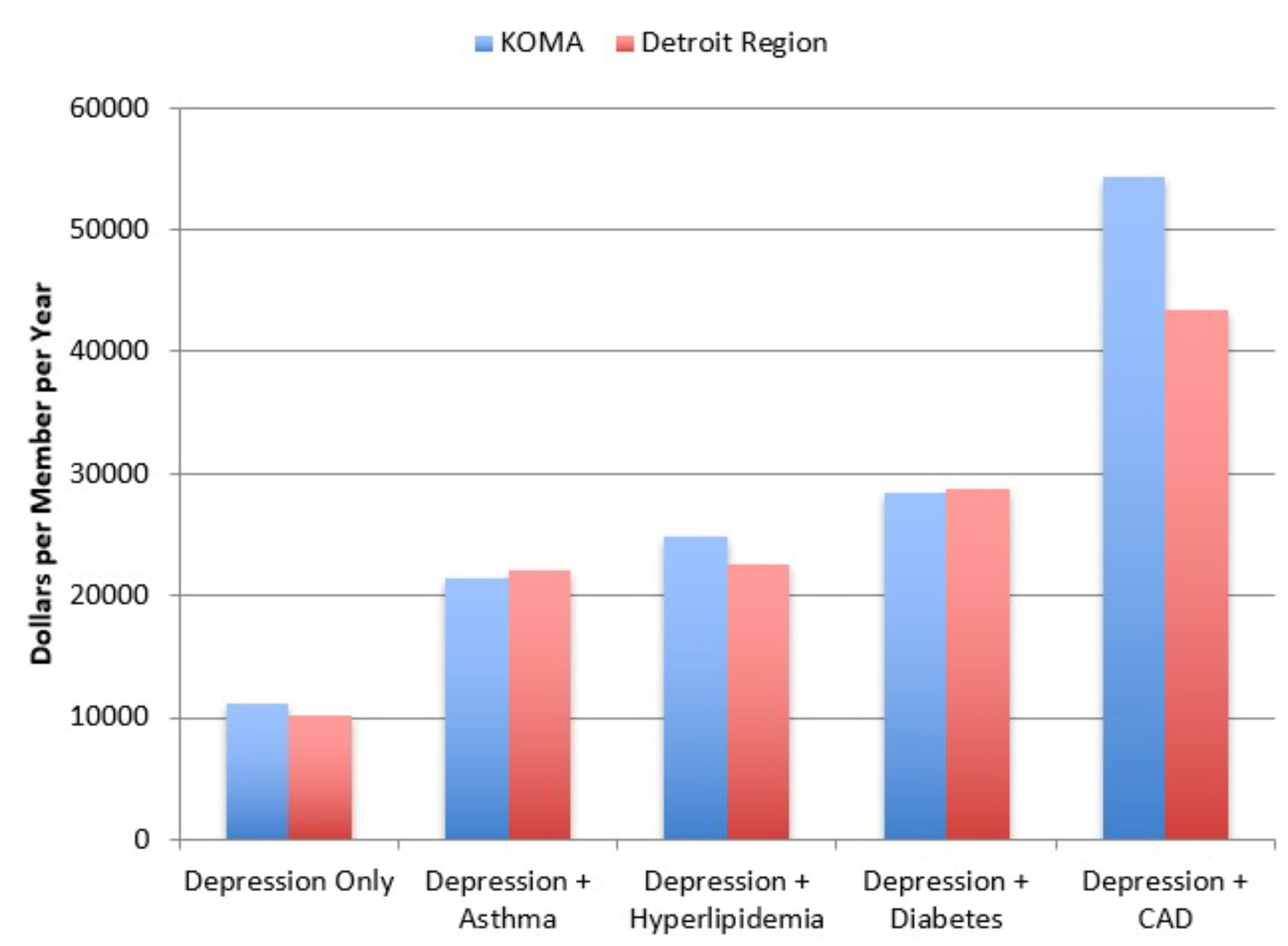
Description: The Expenditures on Members with Depression and Comorbidities, 2023 graph shows the average 2023 insurer expenditures in both KOMA and Detroit regions for each member with only a depression diagnosis, as well as depression in combination with asthma, hyperlipidemia, diabetes, and coronary artery disease. For both regions, combinations of conditions result in expenditure greater than for members with each condition separately.
Source: BCBSM, BCN, and Priority Health member data (2024).
Lastly, looking across Figures 5a and 5b we further note that expenditures for comorbidities do not appear to be additive. That is, average expenditures for members who suffer from both diabetes and depression are higher than if we simply added the average expenditure of a member who suffers from only diabetes with the average expenditure of a member diagnosed with only depression. For KOMA in 2023, the expenditure difference adds up to about $807 (far down from $4,236 in 2022), while the same difference is larger at $4,761 in the Detroit region, down from $7,907 in 2022.
Technical Notes
[1] Analysis of expenditures in previous Health Check reports was based on total allowable expenses for members with prescription coverage. While this variable is present in this year’s data for BCBSM and BCN, it is not present for PH due to a coding change. As an alternative, we used PH data from the year 2018 to estimate the share of total allowable expenses incurred among members without prescription coverage as a linear function of the share of total member months that were without prescription coverage. Only member ZIP codes from 2018 with a share of uncovered months between 0 and 1 were used for the estimation. The model fit the 2018 data well (R2 = 0.701) and the estimated coefficients were used to produce predicted shares for the 2023 data. The predicted shares were used to build total allowable expenses for members with prescription coverage for the member ZIP codes in 2023 with a share of uncovered months between 0 and 1 (25 percent of observations). For the remaining 75 percent, the share was inferred as 1 for member ZIP codes with no covered months and 0 for member ZIP codes where all months had prescription coverage.
References
Ji, L., & Liu. F. (2007). HMO versus non-HMO private managed care plans: An investigation on pre-switch consumption. Health Care Management Science, 10(1), 67-80.
Nicholson, S., Bundorf, K., Stein, R.M., & Polsky, D. (2004). The magnitude and nature of risk selection in employer- sponsored health plans. Health Services Research, 39(6 pt. 1), 1817-1838.
Schaefer, E., & Reschovsky. J.D. (2002). Are HMO enrollees healthier than others? Results from the Community Tracking Study. Health Affairs, 21(3), 249-258.
Tchernis, R., Normand, S.T., Pakes, J., Gaccione, P., & Newhouse. J.P. (2006). Selection and plan switching behavior. Inquiry, 43(1), 10-22.

Daniel Montanera, Ph.D., Assistant Professor, Department of Economics